How to Prepare for a DEXA Body Composition Scan: What to Eat, Wear, and Avoid
How to Prepare for a DEXA Scan | Body Fat USA
How to Prepare for a DEXA Body Composition Scan: What to Eat, Wear, and Avoid
A DEXA body composition scan does not require an elaborate preparation routine. You do not need to dehydrate yourself, complete an aggressive fast, or manipulate your weight before the appointment.
However, food, hydration, exercise, clothing, and the time of day can influence some of the measurements reported by a body composition scan. Following a consistent preparation routine is especially important when you plan to compare multiple scans over time.
This guide explains how to prepare for a DEXA scan, including what to eat, how much water to drink, whether you should exercise, what to wear, and what information you should provide before your appointment.
Why Preparation Affects Body Composition Results
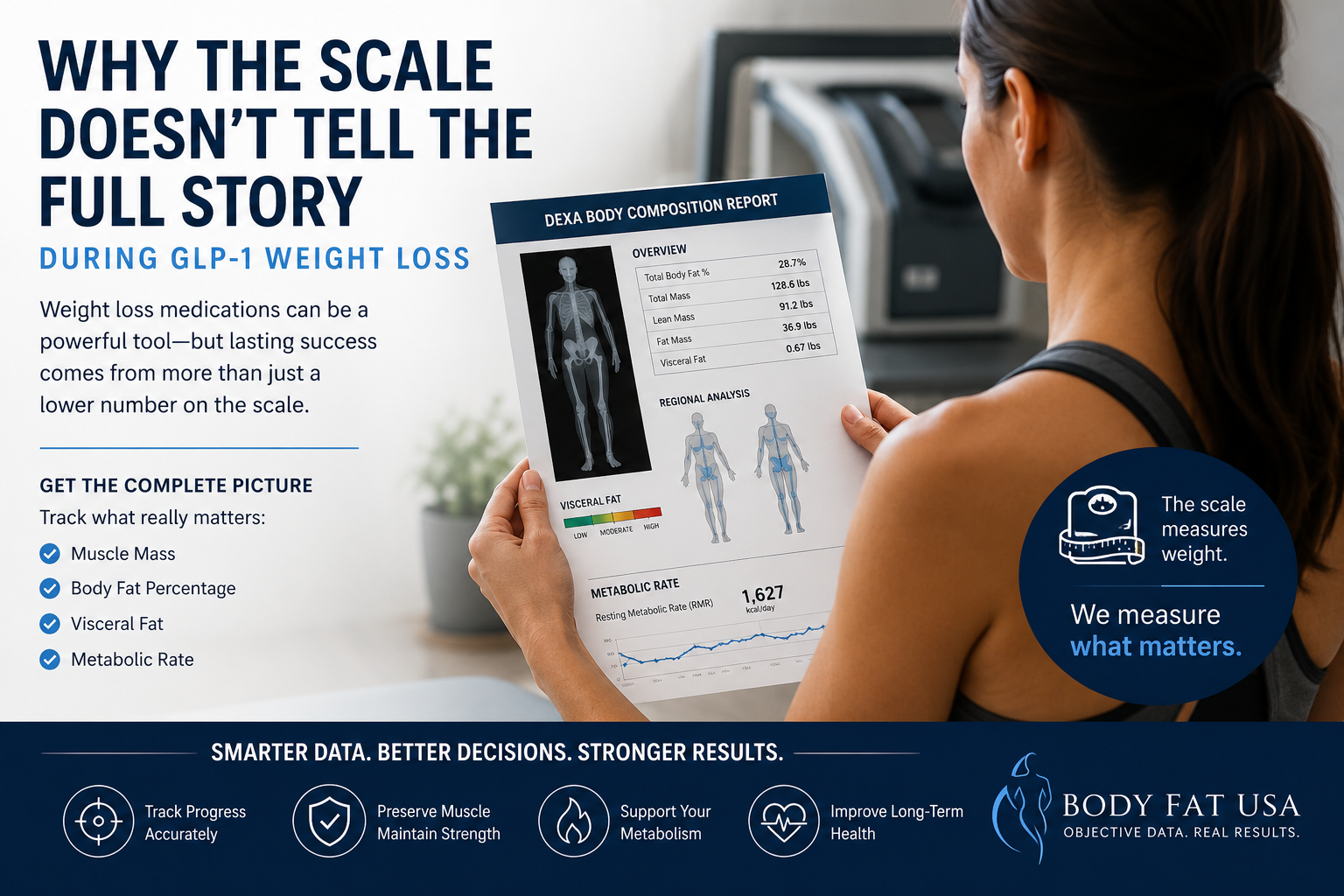
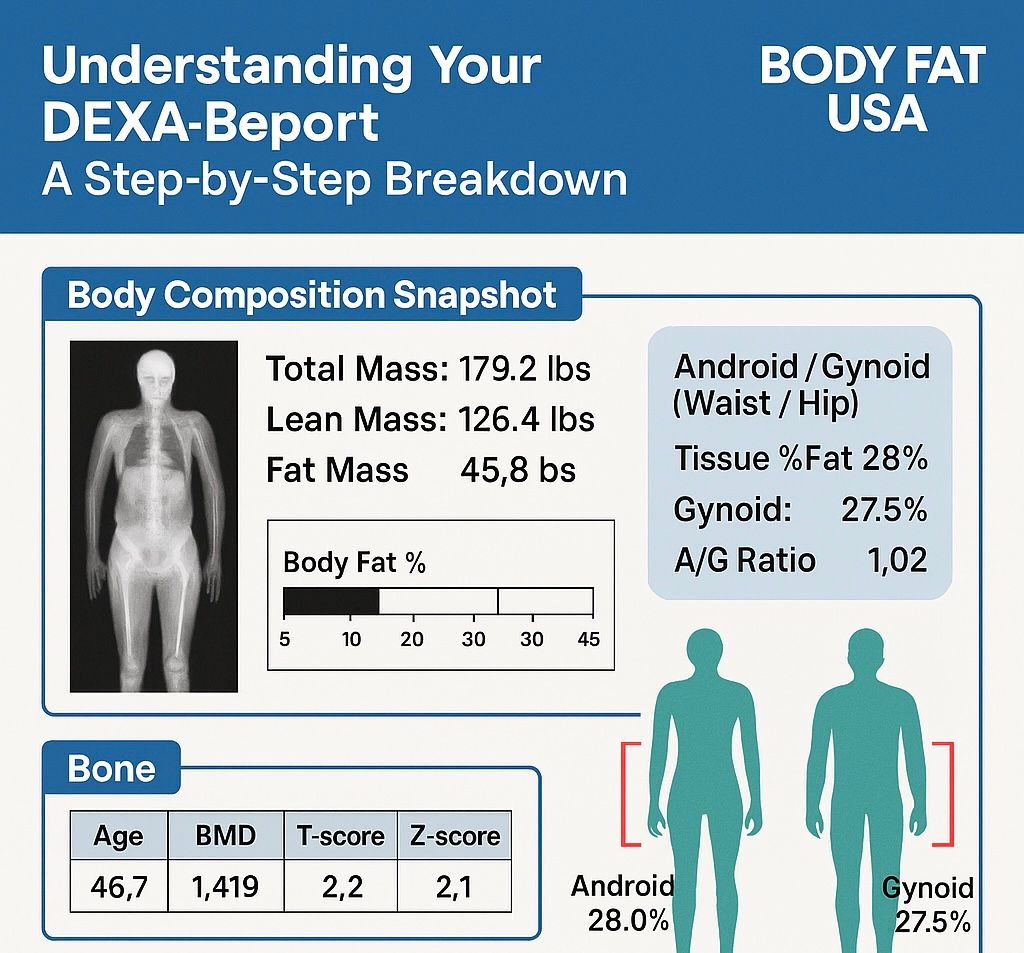
A DEXA scan uses two low-dose X-ray energies to measure and report three primary components of your body:
- Fat mass
- Lean tissue mass
- Bone mineral content
DEXA-derived lean tissue includes water and other nonfat soft tissue. Because hydration, food intake, glycogen storage, inflammation, and recent exercise can change the amount of fluid and material present in the body, they may cause small short-term differences in reported lean mass or body-fat percentage. Research has found that even drinking 500 milliliters of water immediately before a scan can produce a small increase in measured fat-free mass and a corresponding decrease in body-fat percentage.
That does not mean the scan becomes inaccurate simply because you ate breakfast or drank water. The larger issue is comparability.
For example, comparing a morning scan performed before breakfast with an afternoon scan performed after lunch, a workout, and several bottles of water may introduce short-term differences that are unrelated to actual fat loss or muscle gain.
For the clearest trend information, try to arrive under similar conditions each time.
What to Do During the 24 Hours Before Your DEXA Scan
You do not need to change your normal lifestyle the day before your appointment. In fact, attempting to manipulate the result can make the scan less useful.
During the 24 hours before your scan:
- Eat approximately the way you normally eat.
- Maintain your normal fluid intake.
- Avoid intentionally dehydrating or overhydrating.
- Avoid an unusually strenuous workout.
- Avoid dramatic changes in carbohydrate or sodium intake.
- Get a normal amount of sleep when possible.
A particularly hard training session can temporarily affect fluid distribution and inflammation within exercised muscles. Research has specifically examined whether an acute strength and conditioning session can alter DXA-derived body composition results, which supports keeping pre-scan exercise conditions consistent.
Ordinary daily movement is not a problem. The goal is simply to avoid arriving immediately after a demanding workout that is substantially different from the conditions surrounding your previous scan.
Can You Eat Before a DEXA Scan?
For a DEXA body composition scan by itself, you generally do not need to complete a prolonged or aggressive fast.
However, a large meal adds food and fluid to your gastrointestinal system and may slightly affect your body weight and soft-tissue measurements. For that reason, it is best to avoid eating a heavy meal immediately before your appointment.
A practical approach is to:
- Avoid a large meal for approximately two to four hours before the scan.
- Eat a light meal if needed.
- Follow roughly the same meal timing before future scans.
- Avoid intentionally fasting for an unusually long period solely to obtain a lower weight or body-fat result.
The objective is not to arrive as light as possible. The objective is to establish a realistic, repeatable measurement.
What if You Are Also Receiving an RMR Test?
A Resting Metabolic Rate test has stricter preparation requirements than a DEXA scan.
For a Body Fat USA RMR appointment, you should:
- Fast for at least four hours before the test.
- Consume only water during the fasting period.
- Avoid exercise on the day of the test.
- Minimize unnecessary physical activity and stress before testing.
When your appointment includes both DEXA and RMR testing, follow the RMR preparation instructions.
Learn more about Resting Metabolic Rate testing at Body Fat USA.
Hydration Before a DEXA Scan
Arrive normally hydrated.
Do not restrict water in an attempt to lower your scale weight, and do not drink an unusually large volume immediately before the appointment. Both dehydration and overhydration can affect the water contained within lean soft tissue and make comparisons less consistent.
A good preparation strategy is to:
- Drink water normally during the preceding day.
- Continue normal water intake on the morning of your scan.
- Avoid rapidly drinking a large bottle of water immediately beforehand.
- Use the restroom shortly before the scan when possible.
If you are returning for a follow-up scan, try to repeat the same general hydration routine you followed before the first appointment.
Should You Exercise Before a DEXA Scan?
It is best to avoid strenuous exercise before your appointment.
When practical, avoid exercise for approximately 12 hours before the scan and avoid especially heavy training during the preceding 24 hours. Similar recommendations are used by university-based body composition testing programs to improve standardization between measurements.
Exercise may temporarily change:
- Muscle blood flow
- Glycogen and water storage
- Local inflammation
- Fluid distribution
- Gastrointestinal contents
- Perspiration and hydration status
These changes do not represent instant muscle gain or fat loss, but they may influence short-term body composition measurements.
A relaxed walk or normal daily activity is unlikely to create a meaningful problem. The primary concern is completing a hard strength session, long run, intense cycling workout, hot yoga class, or similar activity shortly before being scanned.
What to Wear for a DEXA Scan
Wear comfortable, lightweight clothing containing as little metal as possible.
Good options include:
- Athletic shorts
- Leggings without metal components
- Sweatpants with a drawstring
- A T-shirt
- A sports bra without underwire or metal clasps
- Socks
Try to avoid:
- Metal zippers
- Large snaps or buttons
- Rivets
- Belt buckles
- Underwire bras
- Clothing with decorative metal
- Heavy jewelry
Before the scan, you may be asked to remove:
- Your watch
- Belt
- Keys
- Wallet
- Phone
- Coins
- Jewelry
- Removable accessories
- Items stored in your pockets
Metal-free clothing helps prevent external objects from appearing in the scan image or interfering with the analysis. University testing guidance similarly recommends comfortable clothing without zippers, clasps, rivets, or buckles.
If your clothing contains metal, contact Body Fat USA before the appointment or bring a metal-free alternative.
Pregnancy, Radiation Treatment, and Recent Contrast Procedures
DEXA uses a very low dose of ionizing radiation. Even though the exposure is minimal, certain circumstances require additional precautions.
Pregnancy
You cannot receive a DEXA scan at Body Fat USA if you are pregnant or believe you may be pregnant.
Contact us before your appointment if there is any possibility of pregnancy.
Current Radiation Treatment
Individuals currently undergoing radiation treatment cannot receive a DEXA scan at Body Fat USA. An RMR test may still be available because it does not use radiation.
Contrast Dye, Barium, and Nuclear Medicine Procedures
Contact Body Fat USA before your appointment if you recently had:
- A CT scan involving contrast dye
- A procedure involving barium
- A nuclear medicine scan
- A radioactive tracer
- Another recent imaging procedure involving contrast material
Residual contrast or tracer material can sometimes appear on a DEXA image or interfere with analysis. Some testing programs recommend waiting after contrast-enhanced or nuclear medicine procedures, but the appropriate timing depends on the procedure and material used.
Do not cancel automatically. Contact us with the procedure date and type so we can determine whether the appointment should be rescheduled.
What About Implants or Metal Inside the Body?
Joint replacements, surgical hardware, implanted medical devices, and other internal metal do not prevent a DEXA scan.
However, you should disclose them on your intake form and tell the technician before the scan. Depending on the location and type of hardware, it may appear in the scan image or affect regional analysis.
Do not remove or discontinue any medical device or medication unless instructed by your healthcare provider.
How to Standardize Repeat DEXA Scans
One DEXA scan provides a detailed baseline. Follow-up scans become more valuable when the testing conditions are reasonably consistent.
For repeat scans, try to:
- Use the same facility and scanner.
Measurements from different manufacturers or scanner models are not always directly interchangeable. Research comparing GE Lunar and Hologic systems has found differences that can complicate cross-machine comparisons. - Schedule at a similar time of day.
A 7:00 a.m. scan and a 3:00 p.m. scan may reflect different amounts of food, fluid, and activity. - Follow a similar meal routine.
Try to eat, or not eat, on approximately the same schedule before each appointment. - Maintain similar hydration.
Avoid comparing one scan performed while dehydrated with another performed after unusually high fluid intake. - Use the restroom before scanning.
This reduces one source of short-term body-weight variation. - Repeat your exercise routine.
Avoid completing a hard workout before one scan when you rested before the other. - Wear similar lightweight clothing.
This helps reduce unnecessary variation in scale weight and makes appointment preparation easier. - Avoid deliberate manipulation.
Saunas, dehydration, prolonged fasting, carbohydrate depletion, or last-minute “cutting” may change the number without representing a sustainable change in body composition.
Consistency is more valuable than trying to manufacture the lowest possible body-fat percentage.